Good morning from Cinque Terre! This will be my final deep dive of the month since I’m (sadly) returning back to the States this week. Healthcare Huddle will return to business-as-usual with the weekly breakdowns on the happenings in healthcare.
In case you missed it, here were my previous deep dives over the last two weeks: - Graying America: despite the population 65 and older growing and growing, the number of doctors needed to take care of them isn’t.
-
Counting Sheep: We spend one-third of our life sleeping but don’t give sleep the respect it deserves.
This week, I’ll discuss a topic near and dear to my heart: inefficient patient scheduling.
Before we dive in, you’ll note that the Healthcare Huddle referral program is back up and running in today's newsletter!
Are you new to healthcare? Or just want to refresh your understanding? The guide I put together as a referral reward will provide you all the info you need like "what is insurance?" or "how do doctors make money?" allowing you to have thoughtful discussions about U.S. healthcare.
Just refer friends or colleagues by following the directions in the referral section at the bottom of the newsletter and you’ll be gtg. Ok, now let’s dive in. |
Was this email forwarded to you?
|
|
|
What are you waiting for? |
An appointment with my dermatologist—that’s who I’m waiting for. I called my dermatologist’s office to make an appointment for a routine body check, hoping to get an appointment in a week or two. “A week or two? The next available appointment is in three months. Which day works best for you?” “But… I don’t know what my schedule will be in three months. ”
“Perfect… we’ll just schedule you in whenever then.”
That’s three months between scheduling my appointment to my actual appointment date, what’s known as a lead time. You likely understand the frustration of scheduling a timely appointment with a specialist.
I’m all about efficiency and effectiveness—I see my world through the lens of process maps. So, during my Master’s program in Healthcare Systems Engineering in 2019, my best friend and fellow Huddler, Jonny Blum, and I set out to understand why it takes so long to schedule an appointment with a specialist and what we can do about it. The Deets Let’s talk about a perfect reality: - There are no appointment cancellations
-
There are no no-shows
- There are no walk-ins (since there are no free openings if each patient arrives on time, as scheduled).
- The physician takes advantage of the full-time slot allocated for each patient.
In our reality, 10% of patients fail to show up to their scheduled appointments and 20% of patients cancel their scheduled appointments. Despite the number of appointments that become available from such no-shows and cancellations, patients wait on average 24-days to obtain an appointment. This wait time may exceed 100 days depending on the market size.
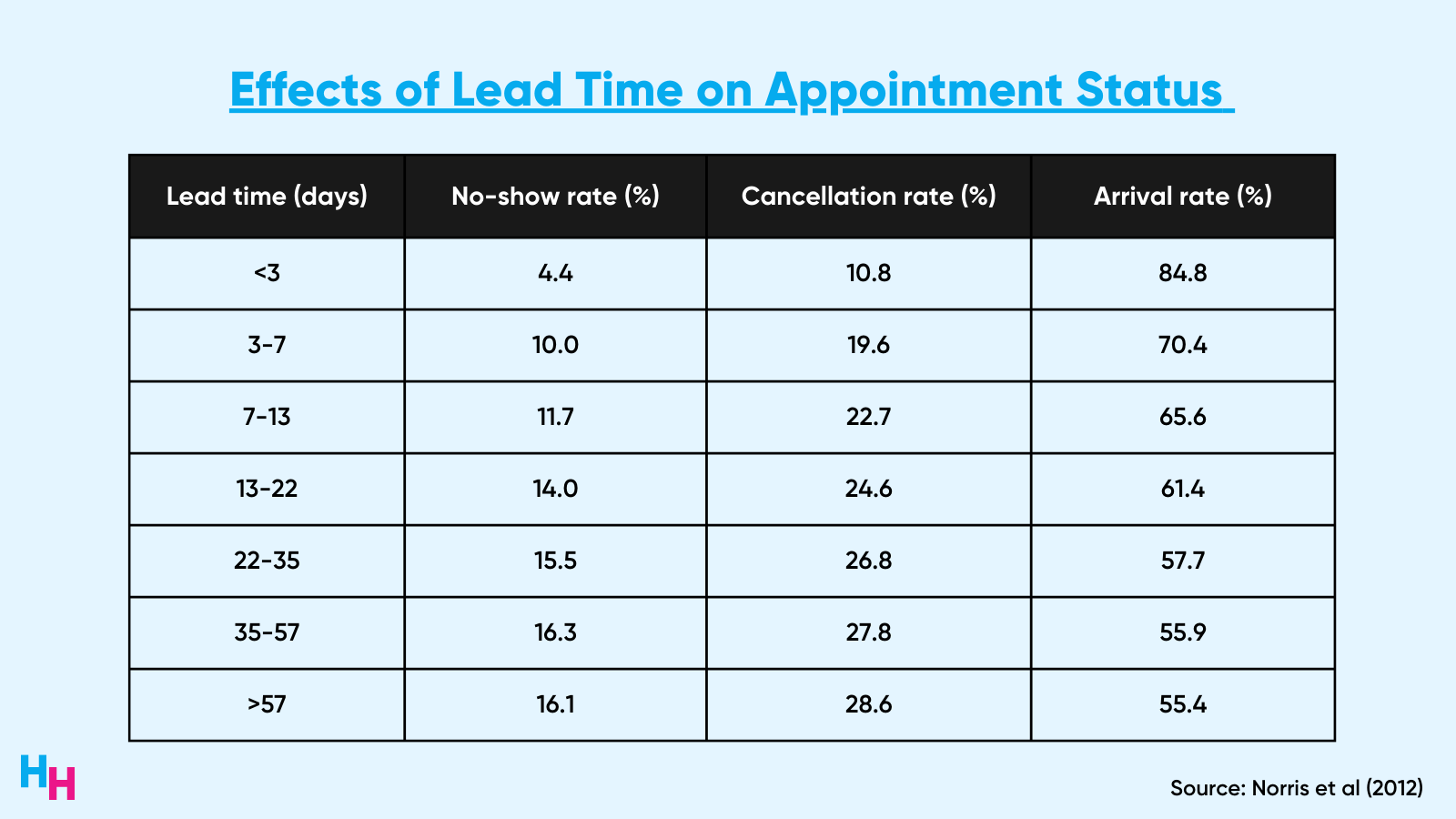
The irony is that there’s a positive correlation between cancellations/no-shows and lengthy lead times. That is, offices that schedule patients far in advance to fill future slots are actually doing a disservice because longer lead times increase the chances of no-shows and cancellations. For example, a lead time of over 55 days results in a 16% no-show rate and 29% cancellation rate.
|
In reality, the efficiency and utilization of obtaining a reasonable appointment time within the U.S. healthcare system is far from an ideal scenario. So What? Patients and doctors experience significant negative consequences of cancellations, no-shows and long wait times to schedule appointments. Long wait times to schedule an appointment for specialty care are associated with lower compliance, worse medical outcomes and increased patient dissatisfaction.
For physicians, no-shows and cancellations lead to decreased efficiency in the practice. In one study by Moore and colleagues (2001), over the course of the year, revenue shortfalls due to cancellations and no-shows at a practice could range from 3%, assuming replacement of all scheduled patients by walk-ins, to 14%, assuming the level of replacement encountered in this study. The projected loss of revenue across 250 working days per year would be more than $350,000. Now, imagine how large this number would be if all clinics in the U.S. were included.
Current Solutions
Jonny and I interviewed dozens of specialty practices, ranging from dermatology to ENT, to better understand their scheduling processes. The lead times ranged from two weeks to six months and each office reported that daily no-shows and cancellations were the norms. When we asked how they deal with patients wanting earlier appointments, they said they maintain a waitlist.
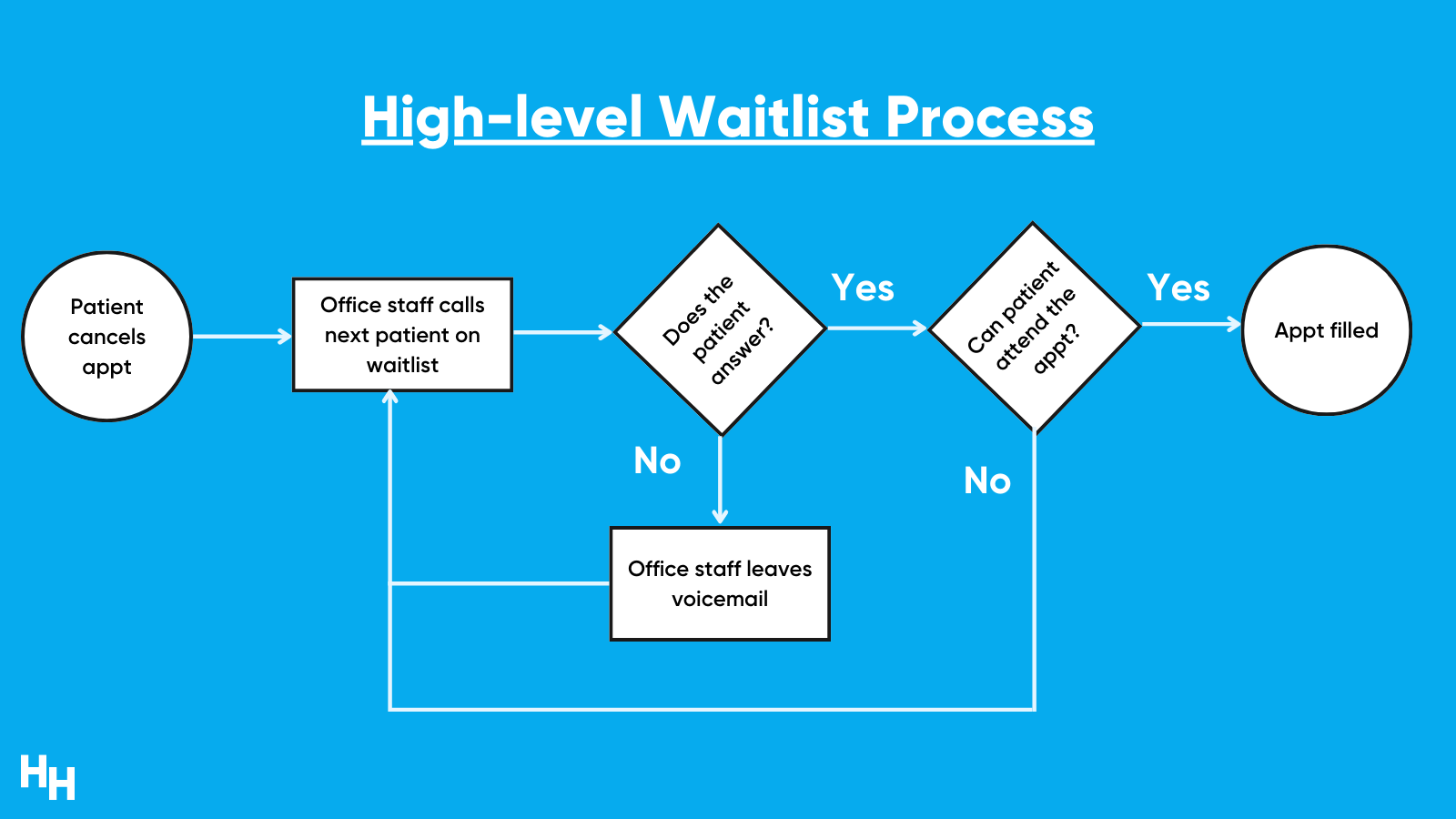
These waitlists varied from excel spreadsheets to paper binders where the office staff would write down the patient’s name and phone number. When there was a cancellation or no-show, the office would go to their waitlist and successively call the patients on it. No answer? Leave a voicemail and proceed to the next patient until one of them answers and confirms the new appointment. This is absurdly inefficient. |
Solution There are a couple of root causes of the no-show and cancellation problem, depending on the perspective you’re analyzing: the patient or the office. Jonny and I focused on no-shows/cancellations accompanied by pages-long waitlists from the office’s perspective.
The solution I want to focus on is automating the manual waitlist process. That is, office staff working their way through long waitlists to call patients to fill in new openings. The automation entails sending automated text messages to patients on the waitlist as soon as a no-show or cancellation occurs. After five minutes of no answer from the patient on the waitlist, the next patient in line receives the text message, and so forth. Regarding technicalities, the automation can work as a standalone platform or integrate into the EHR. The former may add minimally more friction to the workflow of the office staff while the latter would require substantial investor funding to build a team of engineers (trust me, we looked deep into this). Jonny and I created a simulation model to demonstrate the financial consequences of no-shows and cancellations based on data from the literature and the effects of automation. You can access the model on your computer and play around with it by clicking the button below (please make a copy of the Google Sheet). |
Within the model, comments are embedded in the cells to elaborate on certain calculations and definitions. Additionally, any italicized and underlined cell is hyperlinked to the “Assumptions” tab. Anyone experimenting with this model can manipulate the inputs on the “Dashboard” tab. Changing the inputs will change the values shown in the graphs.
Automating the process gives patients quicker access to health care while filling in openings in the office’s schedule that would have been otherwise vacant. Compared to baseline data for a typical dermatology office (see image below for some assumptions made), automating the waitlist process can decrease time spent on reminder calls by the office staff from 160 hours to under 20 hours annually. Additionally, since this model assumes automation is effective at filling in open appointments with patients who want earlier ones, 95% of all appointments will be filled and recovered, resulting in a $250,000 revenue increase annually.
There are a handful of companies tackling this inefficiency. Give them a look:
Take Home Message There are more inefficiencies in the U.S. healthcare system than there are cockroaches in New York City. -
If you don’t believe there could be so many cockroaches in NYC, then you have a solid understanding of this healthcare system.
- However, if you don’t believe there could be so many inefficiencies in this system, then you need to visit NYC.
P.S.
Investigating patient wait times and inefficiencies was part of my capstone project at Lehigh University during my master's program in Healthcare Systems Engineering. It was destined to turn into a full time venture called Nayroo, but once I started medical school, I quickly learned how hard it’d be to balance studies and operations. So, we had to put Nayroo on the shelf.
Either way, I learned so much about this healthcare system through the program and the capstone project—there would be no Healthcare Huddle without this program… think about that for a second.
Many thanks to my professors who advised on the project, Professors Ana Alexandrescu, Terry Theman, Robert McDonald.
And of course, I need to shout out Jonny Blum, Lewis Lazarus, Dan Berkowitz and Adam Sugarman who all played essential roles in the research and prototyping of the project, Nayroo.
|
|
|
-
An empirical investigation into factors affecting patient cancellations and no-shows at outpatient clinics (link).
- Waiting Your Turn: Wait Times for Health Care in Canada, 2020 Report (link).
-
Prevalence, predictors and economic consequences of no-shows (link).
- Appointment scheduling in health care: Challenges and opportunities (link).
-
Sick of waiting: Does waiting for elective treatment cause sickness absence? (link).
|
|
|
Here are some jobs that I’m curating for the healthcare industry. Use this link to submit your role to be featured if you’re looking to hire. Research Coordinator, Noom
Noom is a psychology-based digital health platform that provides intelligent nutrition and exercise coaching. As a research coordinator, you’ll implement studies that support Noom’s ambitious research roadmap.
Healthcare Brand Partner, Workweek
Blake and I are looking for someone to lead our healthcare brand partnerships. We’re looking for someone with B2B media sales experience, specifically in the healthcare space. If you fit this description or know anyone who does, please consider applying to join this excellent company.
Clinical Health Cancer Psychologist, Mayo Clinic
Mayo Clinic, one of the most renowned health systems in the world, is looking for a Clinical Health Cancer Psychologist. This job is undoubtedly rewarding and fulfilling. |
|
|
-
😭 Are children too “soft”? We always hear from older generations that the younger generation has it “too easy,” “complains too much” and “too soft.” Turns out, this has no merit.
-
Penn State 🤝WHOOP: PSU’s student athletes and WHOOP are partnering up!
- 🍷Chianti Wine: I’m no wine expert, but must say the history of Chianti wine is fascinating.
-
🌅 Last Stop in Italy: I’m spending my last few days of my honeymoon in Manarola, Italy. Doesn’t get more beautiful than this! Here’s a picture I took:
|
|
|
SHARE HEALTHCARE HUDDLE, GET EXCLUSIVE CONTENT |
If you share Healthcare Huddle with just 2 friends, I'll personally send you my Healthcare 101 Guide. From the guide, you'll have all the info you need like "what is insurance?" or "how do doctors make money?" allowing you to have thoughtful discussions about U.S. healthcare. |
Once you share Healthcare Huddle with 2 others and they subscribe, you'll get immediate access to my guide!
You can copy and share your link here: {{profile.vars.rh_reflink_5}} Or share via: |
P.S. You have referred {{profile.vars.rh_totref_5}} people so far!
|
|
|
If you have any questions or want to chat about this topic, reply back to this email! Keeping it simple, Jared |
|
|
Want your message in front of 13,500 doctors, nurses and healthcare decision-makers? |
Workweek Media Inc.
2952 Higgins Street
Austin, TX 78722 Want to ruin my day? Unsubscribe. |
|
|
|