{if hosp_dorm_120 == true}
Quick favor: Our records indicate that you aren’t opening this email. But records can be wrong. Please click here if you’d like to remain subscribed to Hospitalogy. | |
|
{/if}{if profile.vars.hew_transition}
A reminder: You’re receiving this because you were previously subscribed to HealthExecWire. Hope you enjoy. | |
|
{/if}
Happy Tuesday Hospitalogists,
We are BACK in March Madness! Join the Hospitalogy 2026 March Madness Bracket Challenge HERE - I’ll shout out and exclusively interview the winner on their bracket picking strategies once a champion is crowned. (If you choose Texas to lose to NC State you’re out though.) With that out of the way, we’re talking about the problems in healthcare that we keep trying to solve with technology when they’re really leadership or incentive issues, the AHA’s Costs of Caring 2026 report, and AdventHealth’s creation of a new primary care division. Enjoy! |
Was this email forwarded to you? |
|
|
Technology vs Leadership Issues |
|
|
What problem in healthcare do we keep trying to solve with technology that’s really a leadership or incentive issue? |
|
|
THE CLINICIAN BURNOUT TAKE |
Anonymous “I think clinician burnout is bigger than technology can fix.
That's not to say technology hasn't helped. We implemented AI scribing and that's worked out well. Now we're piloting AI for clinical documentation and that's really cutting down on after-hours work. But I think we're just making documentation faster while avoiding harder leadership questions: Why do we tolerate unnecessary documentation in the first place?
Why are clinicians still the system’s integration layer? Why do we reward volume and compliance over judgment and outcomes? Technology can reduce pain at the margins, but burnout persists because incentives still reward throughput, defensive documentation, and risk transfer, not thoughtful care delivery.
I hate to say it, but the same pattern shows up in patient experience. We invest in digital front doors and chatbots, but the experience breaks when pricing isn't as transparent as promised, networks change mid-year, or access disappears because of contract disputes. Those are governance and incentive problems, not UX failures.” |
Anonymous
“Prior authorization, patient access, and revenue cycle complexity. We’ve layered on portals, AI tools, automation, and workflows to optimize systems that are fundamentally designed to create friction. No amount of technology can fix a model where payers are incentivized to delay or deny care, providers are penalized for compliance failures they don’t control, and patients are left navigating the fallout.” |
THE MISALIGNED INCENTIVES TAKE |
Anonymous
“We keep trying to solve misaligned incentives with technology. That almost never works the way we hope.
Healthcare loves to throw software at problems that are fundamentally about who gets paid, who bears risk, and who owns outcomes. Prior auth is the obvious example. We’ve layered automation, AI, and analytics onto a process that exists because payors and providers don’t trust each other’s incentives. Faster denials, smarter denials, automated appeals. There is a lot to be said for technology making processes smoother. But none of that fixes the core issue.
Same with care coordination, value-based care, and even clinician burnout. We deploy tools to ‘optimize workflows’ while leaving leadership structures, compensation models, and accountability unchanged. Yes, tech can amplify clarity, but it can’t create it.
Leaders need to be willing to realign incentives, financially and operationally. Without that, even technology that has massive potential could wind up just accelerating the friction that's already there.” |
Kat Lewis - Community Manager
“Coming from marketing, this question REALLY resonates. In teams I’ve been part of, we’ve tried to use tech to fix problems that were ultimately about leadership, incentives, and what people are rewarded for. The tech usually does exactly what it’s told to do, it just reflects the system behind it. Feels like a cross-industry pattern.” |
Anonymous
“Physician productivity, risk coding and reduction of avoidable utilizations.”
Hospitalogy members can join this discussion here. Not a member yet? Apply to join here. |
|
|
The Real Drivers of Hospital Cost Growth |
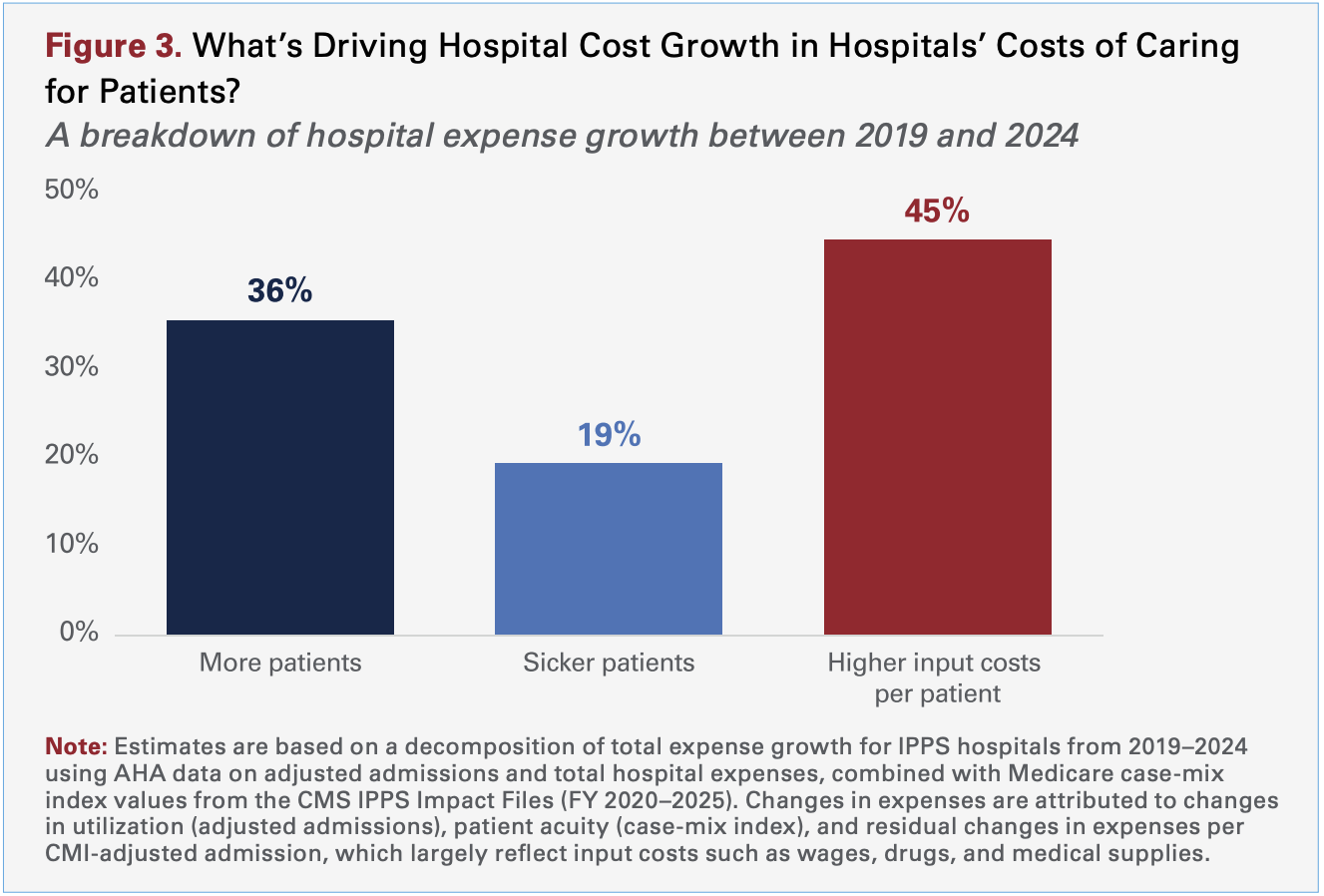
The AHA has released its Costs of Caring 2026 report, a breakdown of what’s actually driving hospital costs in 2026.
The report shows hospitals are treating more patients who are significantly sicker, while the core inputs required to care for them, such as labor, drugs, and medical supplies, are rising faster than reimbursement.
Key takeaways include: - Total hospital expenses grew 7.5% in 2025, more than double the rate of hospital price growth (3.3%).
- Hospital workforce costs now exceed $1T annually.
- Drug prices are growing 4x faster than hospital prices.
- Hospital drug expenses increased 13.6% in 2025 (for academic medical centers, the increase was 21.6%).
-
Hospitals spent roughly $30B in 2025 on technology and services to protect against cyber threats.
- Hospitals spent $43B in 2025 trying to collect payments insurers owed, including nearly $18B just overturning claims denials.
-
56.1% of hospital costs are tied to service lines where reimbursement doesn’t cover the cost of care, including behavioral health, obstetrics, infectious disease services, and burns and wounds.
For health system leaders, the full report is a useful breakdown of the structural forces reshaping hospital economics, and why cost growth isn’t just about hospital prices. Read it here. |
A major health system has started deploying Tom, Lumeris' AI primary care as a service platform across its system. Not a pilot. A long-term enterprise deployment. While most health systems are still running point solution experiments, forward thinkers are betting AI-enabled primary care is how you grow the front door, expand panels, and capture downstream value — without burdening your system with more real estate overhead or headcount that doesn’t exist in your market.
First movers in AI primary care will eat market share. The question isn't whether this is coming. It's whether you'll be the disruptor or the disrupted. |
Carving Out Primary Care: AdventHealth's Standalone Division Experiment |
Had a blast sitting down with Brent Davis, CEO of AdventHealth's Primary Health Division, for this one (Apple | Spotify). Brent is running what is essentially a startup inside one of the largest health systems in the country — a $500M bet that non-hospital care delivery needs its own operators, its own capital, and its own identity.
We got into the economics of primary care subsidies, how AdventHealth is borrowing consumer analytics from retail giants, the emerging menopause care opportunity, AI pragmatism, a remarkably smooth CEO transition, and a value-based care strategy that starts with AdventHealth being its own first customer. Listen to the full podcast episode (Apple | Spotify). Here’s an executive summary of our convo for those who don’t have the time: -
AdventHealth carved out a $500M, six-year primary health division to run non-hospital businesses outside traditional hospital operator logic — and it's working: subsidy down from ~$150M to ~$110M while visits jumped from 2.4M to 2.9M annually.
-
Consumer segmentation borrowed from retail site-selection analytics (think Target and Home Depot) is driving AdventHealth's primary care model placement — matching urgent care to soccer moms and senior clinics to aging demographics by geography.
-
AdventHealth's CEO transition was a "baton pass, not a rebuild" — new CEO David Banks founded the primary health division himself, giving ambulatory strategy rare C-suite air cover heading into 2026.
-
The system is using its own $1B self-funded health plan as a VBC proving ground before going to market with employer solutions — a quietly powerful move as employers watch healthcare premiums outpace revenue growth 2:1.
|
|
|
-
Read: “After attending HIMSS March 9-12 in Las Vegas, health system CIOs are excited about implementing agentic AI — and getting a return on investment from it — while governance is becoming ‘sexy,’ as one leader put it.” Read more from Becker’s Health IT.
-
Breakdown: Providers taking on financial risk without the actuarial tools to manage it? My article shares how Arbital Health’s AI platform puts actuarial-grade insights into the hands of VBC operators.*
- Event: Join me, Herd Midkiff, and Kyle Kirkpatrick for an executive briefing breaking down the trends reshaping hospital financial performance, and what leaders should be watching next. 3/27 at 12 PM CT. Register here.
*This read is brought to you by one of my brand partners who help make this newsletter possible! |
DON’T FORGET to join the Hospitalogy 2026 Bracket Challenge! Join here on ESPN. I haven’t watched a lick of basketball this year since Texas is borderline awful but I’ll give it the old college try. |
|
|
I would love to know your thoughts! Just reply to this email.
– Blake |
|
|
{if profile.vars.board_room_user_fitness == true}The conversation doesn't have to stop here
Keep learning and connecting in the Hospitalogy Network
EVENTS | FEED | LIBRARY | DIRECTORY
|
|
|
{/if}{if !profile.vars.board_room_user_fitness && profile.vars.board_room_user_fitness != false}I'm building a community of leaders in strategy, finance, and ops
at hospitals and health systems to help us connect, learn, and grow together. |
|
|
{/if}
Get your brand in front of 67,000+ executives and healthcare decision-makers. |
Workweek Media Inc.
1023 Springdale Road, STE 9E
Austin, TX 78721
Want to ruin my day? Unsubscribe. |
|
|
|