
PUBLIC HEALTH
The Other Epidemic
By the time you finish reading this newsletter, at least one American will have died from an opioid overdose.
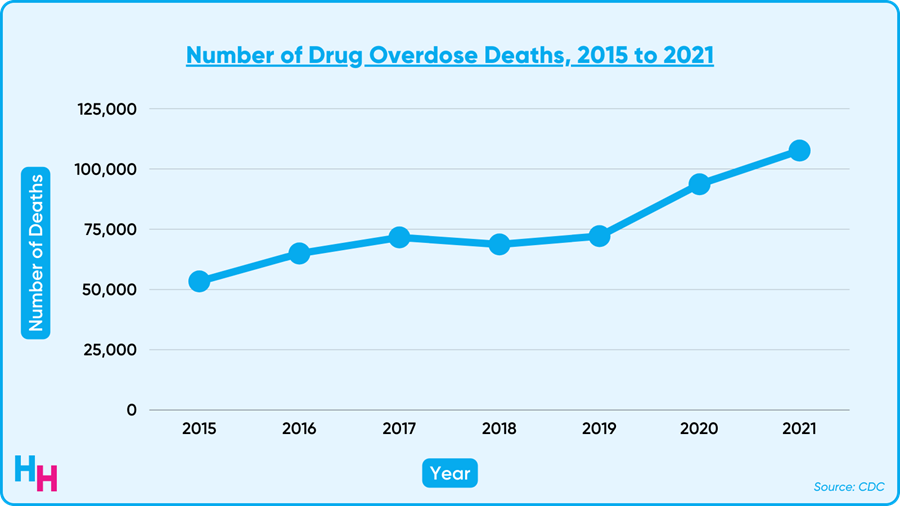
Overdose deaths have increased nearly 50% since the pandemic began, according to new data from the CDC. 2021 alone saw a record 108K overdose deaths, likely driven by fentanyl-laced drugs.
The Deets
While the 108K deaths included all types of drugs, most deaths involved opioids. And of those opioid-related deaths, around 70% were synthetic opioids like fentanyl, which is up to 100x more potent than morphine. The overdose toll on individuals and society is devastating, with young people amassing greater than 1.25 million years of life lost.
What’s particularly concerning is the shift in who is affected by overdose deaths.
- Adolescents: The rate of drug overdose deaths among adolescents was 2.36 per 100K in 2019. In 2021, it was 5.49 per 100K, a 133% increase over two years. Additionally, fentanyl-related deaths among teens increased 250% during that same period, from 1.21 per 100K to 4.23 per 100K. American Indian and Alaska Native teens had the highest overdose death rate (11.79 per 100K), followed by Latinx (6.98 per 100K).
- Race: The overdose mortality gap among Black and white individuals was reversed during the pandemic. Overdose deaths among Black individuals increased from 24.7 per 100K in 2019 to 36.8 per 100K in 2020—16.3% higher than white individuals’ in 2020. A decade earlier, the overdose death rate for white individuals was double that of Black individuals. American Indian or Alaska Native populations still face the most considerable burden of overdose deaths among all races and ethnicities.
My Thoughts
The pandemic has made us numb to catastrophic mortality numbers, allowing us to distance ourselves from the horrific reality of two epidemics: Covid-19 and opioid overdoses. Ironically, one epidemic (Covid-19) has exacerbated the other epidemic (opioid overdoses).
It’s easy to feel hopeless as a provider thinking about the progress—or lack thereof—in helping those with substance use disorder. I believe substance use disorder (addiction) needs to be viewed differently. Instead of thinking of addiction as a “bad habit” that people will eventually “outgrow,” we should consider it like any other chronic disease. Just like patients with type I diabetes need insulin, patients with addiction need access to effective medications and harm reduction measures.
Adopting this mindset requires bridging together old school thought and new school thought.
- Old School: “The goal is to get people to stop using drugs entirely.”
- New School: “The goal is to recognize that ‘stop using drugs entirely’ is often infeasible, and the next best treatment we can provide is medication therapy and harm reduction strategies.”
Combining these two schools of thought requires us to view addiction on a continuum. The continuum starts with abstinence and ends with deleterious. At any point in time, someone with substance use disorder is on this continuum.
In the context of opioid use disorder, someone closer to abstinence may be able to start methadone treatment and taper off. Often, though, patients may need to stay on methadone for the rest of their lives—just like patients with type I diabetes need insulin for the rest of their lives. However, someone closer to the deleterious end may best benefit from harm reduction strategies such as providing them with sterile syringes, drug-checking supplies for safer use, and naloxone to treat opioid overdose.
At the end of the day, “108K overdose deaths in one year” screams that this public health crisis is far from over. Viewing substance use disorder on such a continuum will help providers recognize the complexity of addiction and the different tools we can use to help those in need.

HOSPITALOGY THIS WEEK
Hospitalogy’s Week Ahead
Be on the lookout for the Hospitalogy sends this week! On Tuesday, I’ll be highlighting the Advocate Aurora – Atrium Health merger and other top of mind healthcare news. Deep dive coming on Atrium/Advocate NEXT week.
Then, while I’m in Austin on our first Workweek work retreat, I’ll take you guys down the journey of the 10 worst performing Health Tech & Services stocks from 2021.
See ya Tues & Thurs, Hospitalogy fam.

PHARMA
Join the thousands of healthcare professionals who read Hospitalogy
Subscribe to get expert analysis on healthcare M&A, strategy, finance, and markets.
No spam. Unsubscribe any time.
The Next Frontier of Migraine
Fresh off a profitable fiscal year, Pfizer will use its cash to acquire Biohaven Pharmaceuticals for $11.6B—their largest acquisition since 2016. Biohaven focuses on neurological and neuropsychiatric diseases like migraines, which are often overlooked and untapped in therapeutics.
The Deets
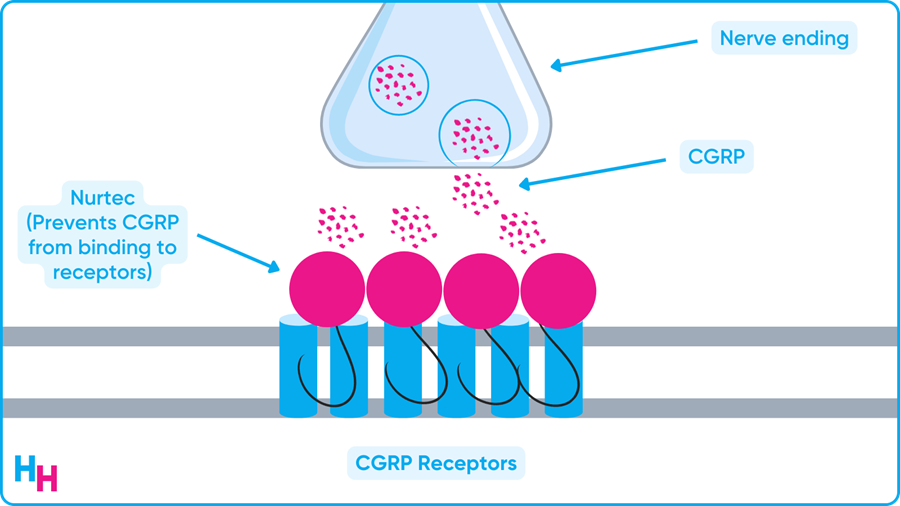
The $11.6B deal will give Pfizer access to Biohaven’s innovative calcitonin gene-related peptide (CGRP)-targeting migraine medications:
- Rimegepant (Nurtec): FDA-approved for prevention and acute treatment of migraines.
- Zavegepant: Recently submitted to FDA for approval. It’s a nasal spray used to prevent and treat migraines.
- Five pre-clinical CGRP medications: Too early to say anything about these drugs, but Pfizer sees potential.
Pfizer plans to broaden Nurtec’s reach to patients, for which there’s a lot of potential—Biohaven estimates Nurtec represents just under 50% of the CGRP drug market. Pfizer, therefore, plans to double Nurtec’s sales team and reach an additional 70K primary care providers and Ob/Gyns.
CGRP and the Next Frontier of Migraine
CGRP is a peptide that modulates neuronal pain and vascular activity and is thought to drive migraines. The above drugs antagonize CGRP receptors, blocking their activity. Other CGRP medications include monoclonal antibodies, which bind to CGRP receptors and also block their activity. Despite being relatively new, CGRP drugs are promising and are another effective tool to prevent or treat migraines.
My Thoughts
Have you ever had a migraine? It’s the worst. I get them when my sleep dips below 7 hours for several nights in a row. I can’t function. Here are three things to know about migraine:
- It’s common, affecting around 12% of the U.S. population, and is 2-3x more common in women than men.
- It’s the number two cause of disability worldwide, and number one among young women.
- It’s a major public health issue that receives little attention.
There are several ways to prevent and treat migraine, including lifestyle changes and medications. Nothing yet has been groundbreaking per se, but drugs targeting CGRP receptors may be what we need—and Pfizer thinks so, too. Given migraine is an often overlooked neuropsychiatric disease, Pfizer may be the “big guy” to start leading the charge into migraine therapeutics.
Regarding digital mental health, there are a few companies targeting migraine prevention and treatment. Cove is one company that caught my eye. With Cove, you can schedule a consultation and get medical treatment (like Nurtec) that fits what you need and what your insurance covers. Similarly, Neurahealth is an app-based platform that tracks your migraine triggers (read: monitoring lifestyle factors) and shares them with a neurologist who can provide a treatment plan.
Overall, migraine is a common, disabling condition worldwide and hasn’t received the attention it needs, in my opinion. However, I think Pfizer’s acquisition of Biohaven may start a “race” to develop the most effective migraine treatment while digital health startups focus on facilitating access to providers and treatments.

OUTSIDE THE HUDDLE
- The VA’s multi-billion-dollar implementation of Cerner’s EHR isn’t going so hot per a recent audit. There have been outages (like the one I told you about in April), and other issues with uploading old records and linking medical device data, just to name a few. EHRs are supposed to improve workflows and make data more accessible, but that’s not always the case.
- The FDA approved Lilly’s diabetes drug tirzepatide. Does the drug’s name sound familiar? I wrote about tirzepatide two weeks ago and its strong weight-loss effects.
- Heart surgeon turned medical misinformation protege Dr. Mehmet Oz has strong prospects of winning Pennsylvania’s Republican Senate primary. But some say this could be good for medicine and tout his track record of spewing “scientifically sound” information, at least compared to the other GOP candidates.
- As Covid-19’s burden on hospitals has eased, so has the demand for travel nurses, some of whom were making up to $10k per week at the height of the pandemic. The average physician made $339,000 in 2021 ($6,519 per week)! While some expect travel nursing to grow, many are seeing contracts cut early and opting for full-time jobs, which some hospitals are incentivizing. Blake wrote a great essay on travel nurses here.
- Offering to turn your medical bill into monthly payments, Walnut raised a $110 million series A. While this doesn’t reduce the overall cost of care for patients, it may help ease the burden for those who end up with unexpected significant medical bills.
- A small city in Texas called Ferris plans to make healthcare free for all using funding from the American Rescue Plan Act. Residents will have access to an app connecting them with around 200 providers. It will be interesting to see the outcomes of this first in the U.S. system, but keep in mind this is a city of just a few thousand people.
